Introduction: The Myth of the Vestigial Organ
For generations, the vermiform appendix was largely dismissed by the medical community as an evolutionary leftover—a useless, vestigial pouch waiting to become infected.
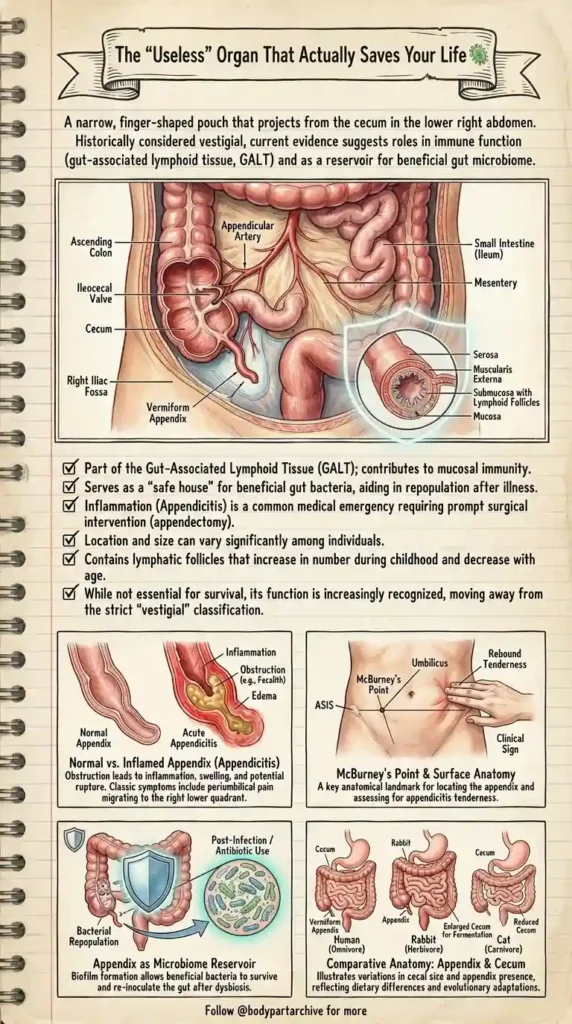
However, modern histology and gastroenterology have drastically changed this narrative. Far from being a ticking time bomb, this narrow, finger-shaped pouch projecting from the cecum plays a highly sophisticated role in your body’s immune defense and digestive recovery. Let’s open the archives and explore the true anatomy of this deeply misunderstood organ.
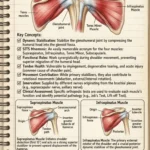
Gross Anatomy and Location
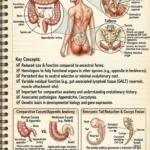
To locate the appendix, we have to look at the junction where the small intestine meets the large intestine.
The terminal end of the small intestine (the Ileum) empties through the Ileocecal Valve into the Cecum, the first pouch of the large intestine. Dangling directly off the cecum in the lower right quadrant of the abdomen is the Appendix. It is highly vascularized, receiving its blood supply directly from the Appendicular Artery. Interestingly, while its base is relatively fixed, its exact location and size can vary significantly among individuals.
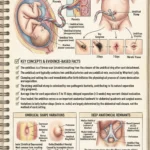
The Safe House: Immunity and the Microbiome
If it’s not useless, what does it actually do? The answer lies under a microscope.
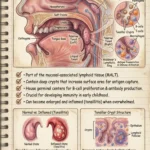
GALT (Gut-Associated Lymphoid Tissue): The submucosa of the appendix is packed with lymphoid follicles. This makes it a vital component of your mucosal immune system, actively helping to detect and defend against intestinal pathogens.
The Microbiome Reservoir: Your gut is filled with trillions of beneficial bacteria necessary for digestion. When you suffer from a severe gastrointestinal illness (like dysentery or cholera), the gut is violently flushed out. Current evidence suggests the appendix serves as a biological “safe house.” It shelters a biofilm of beneficial bacteria, allowing them to survive the illness and rapidly re-inoculate the gut afterward.
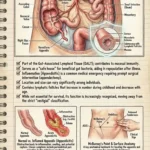
The Medical Emergency: Acute Appendicitis
While it has essential functions, the appendix’s narrow, tube-like structure makes it highly susceptible to obstruction.
When the opening becomes blocked—often by a hardened piece of stool known as a Fecalith—the appendix cannot empty its mucus. This leads to rapid inflammation, severe edema (swelling), and acute bacterial infection. If not treated promptly with an appendectomy (surgical removal), the pressure can cause the organ to rupture, spilling toxic bacteria into the sterile abdominal cavity and causing life-threatening peritonitis.
Clinical Signs: Finding McBurney’s Point
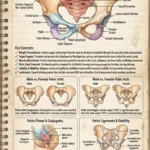
For nursing and medical students, diagnosing appendicitis is a high-yield board exam topic. The classic presentation begins with a dull pain around the umbilicus (belly button) that gradually migrates to the lower right abdomen.
Clinicians use a specific anatomical landmark called McBurney’s Point to assess this. It is located approximately one-third of the distance from the anterior superior iliac spine (ASIS) to the umbilicus. Deep tenderness here, especially “rebound tenderness” (pain that sharply worsens when the examiner releases pressure), is a hallmark clinical sign of acute appendicitis.
Conclusion
It is time to give the appendix the respect it deserves. While you can certainly live without it, its role in mucosal immunity and microbiome preservation proves that the human body rarely holds onto structures without a brilliant physiological reason.