The Brachial Plexus: Simplifying the Med Student’s Ultimate Nightmare
Ask any medical, nursing, or physical therapy student which anatomical structure causes them the most anxiety, and the answer is almost always the same: The Brachial Plexus. This incredibly complex network of nerves is responsible for the cutaneous sensation and motor function of the entire upper limb—including the shoulder, arm, forearm, and hand.
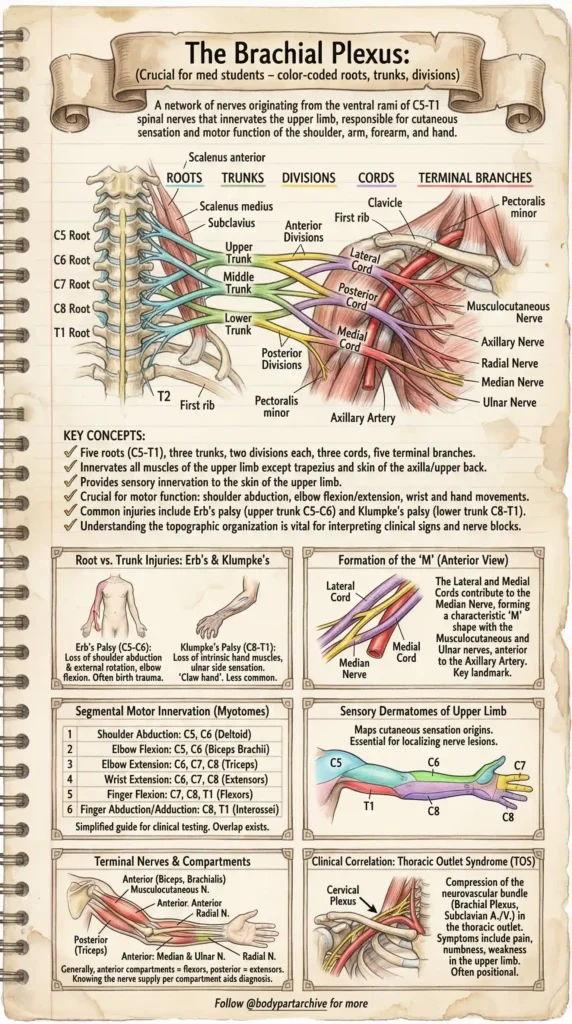
While textbooks often present it as a confusing web of intersecting lines, understanding the topographical organization of the Brachial Plexus is vital for interpreting clinical signs, diagnosing nerve injuries, and performing nerve blocks. Today, we are breaking it down visually, step-by-step, using our premium color-coded anatomy cheat sheet.
The Foundation: Roots, Trunks, Divisions, Cords, and Branches
The secret to mastering the Brachial Plexus is remembering its basic structural flow: Really Tired Drink Coffee Black (Roots, Trunks, Divisions, Cords, Branches).
1. The Roots (C5 – T1)
The plexus begins with the ventral rami of five spinal nerves: C5, C6, C7, C8, and T1. These emerge from the spinal cord, passing between the anterior and middle scalene muscles in the neck.
2. The Trunks (Superior, Middle, Inferior)
Shortly after emerging, these roots merge to form three distinct trunks:
- Superior Trunk: Formed by the union of C5 and C6.
- Middle Trunk: A direct continuation of C7.
- Inferior Trunk: Formed by the union of C8 and T1.
3. The Divisions (Anterior and Posterior)
As the trunks pass behind the clavicle, each one splits into an anterior and a posterior division. This separation is crucial because anterior divisions generally supply flexor muscles, while posterior divisions supply extensor muscles.
4. The Cords (Lateral, Posterior, Medial)
The divisions then reorganize into three cords, which are named based on their anatomical relationship to the axillary artery:
- Lateral Cord: Formed by the anterior divisions of the superior and middle trunks.
- Posterior Cord: Formed by the posterior divisions of all three trunks.
- Medial Cord: Formed by the anterior division of the inferior trunk.
5. Terminal Branches
Finally, the cords give rise to the five major terminal nerves of the upper limb: the Musculocutaneous, Axillary, Radial, Median, and Ulnar nerves.
The Genius “M” Shape Hack:
When looking at the anterior view of a dissected axilla, you can easily identify the terminal branches by finding the characteristic ‘M’ shape. The Lateral and Medial cords converge to form the Median nerve in the center, flanked by the Musculocutaneous nerve laterally and the Ulnar nerve medially.
High-Yield Clinical Correlations
Anatomy is only useful if you can apply it clinically. Here are the major pathologies associated with the Brachial Plexus that frequently appear on board exams (like the USMLE) and in clinical practice.
Erb’s Palsy (Upper Trunk Injury)
Erb’s palsy typically results from an injury to the C5 and C6 nerve roots. This is often caused by a severe downward traction on the shoulder, such as during a difficult childbirth or a motorcycle accident.
- Clinical Presentation: The patient presents with the classic “Waiter’s Tip” posture. There is a loss of shoulder abduction, external rotation, and elbow flexion, leaving the arm hanging limply by the side, medially rotated.
Klumpke’s Palsy (Lower Trunk Injury)
A much less common injury, Klumpke’s palsy affects the C8 and T1 nerve roots. This usually occurs when someone suddenly grabs a branch to stop a fall from a height, or during an upward traction injury at birth.
- Clinical Presentation: Because C8 and T1 primarily innervate the small intrinsic muscles of the hand, this injury results in a characteristic “Claw Hand” deformity and loss of sensation on the ulnar side of the forearm and hand.
Thoracic Outlet Syndrome (TOS)
TOS is a condition where the neurovascular bundle (the Brachial Plexus and the Subclavian artery/vein) gets compressed as it passes through the narrow thoracic outlet—often between the clavicle and the first rib, or due to an extra cervical rib.
- Symptoms: Patients often complain of positional pain, numbness, tingling, and weakness in the upper limb, especially when raising their arms above their head.
Myotomes and Dermatomes: The Clinical Map
To localize nerve lesions efficiently, clinicians rely on myotomes (muscle groups innervated by a single nerve root) and dermatomes (skin areas innervated by a single nerve root).
Key Upper Limb Myotomes:
- C5: Shoulder Abduction (Deltoid)
- C6: Elbow Flexion (Biceps Brachii) / Wrist Extension
- C7: Elbow Extension (Triceps) / Finger Extension
- C8: Finger Flexion
- T1: Finger Abduction/Adduction (Interossei)
Sensory Dermatomes: Mapping cutaneous sensation is equally important. For example, numbness on the lateral aspect of the forearm points toward a C6 issue, while numbness in the pinky finger is a classic C8 indicator.
Conclusion
The Brachial Plexus doesn’t have to be a nightmare. By breaking it down visually into its core components—and understanding the clinical significance of each root and trunk—you can master this high-yield topic with confidence.
Save our vintage anatomical cheat sheet to your study notes, and be sure to check back at BodyPartArchive for more visual guides that make medical science beautiful and easy to understand!