The Rotator Cuff: Mastering the SITS Muscles and Shoulder Anatomy
The human shoulder is a marvel of biomechanical engineering. Unlike the hip joint, which is a deep, highly stable socket, the shoulder (glenohumeral joint) is more like a golf ball sitting on a small tee. This unique design allows for an incredible range of motion—but it comes at a steep cost: a high susceptibility to instability and injury.
So, what keeps your arm from falling out of its socket every time you throw a ball or lift a heavy box? The answer lies in a complex of four relatively small, dynamic stabilizing muscles known collectively as the Rotator Cuff. For medical, nursing, and physical therapy students, mastering these muscles is an absolute necessity. Today, we are breaking down the Rotator Cuff visually using the famous “SITS” mnemonic.
The SITS Mnemonic: Your Anatomy Cheat Code
The easiest way to remember the four muscles of the rotator cuff is by using the acronym SITS:
- S – Supraspinatus
- I – Infraspinatus
- T – Teres Minor
- S – Subscapularis
These muscles originate from various parts of the scapula (shoulder blade) and insert onto the head of the humerus (upper arm bone), effectively wrapping around the joint to form a supportive “cuff.”
Detailed Breakdown of the Four Stabilizers
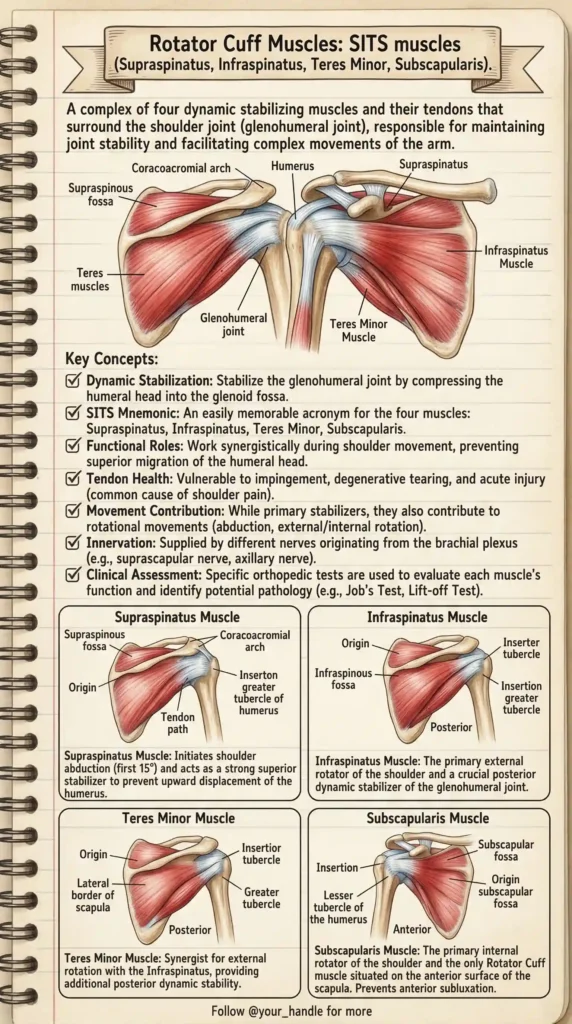
Let’s dive into the origin, insertion, action, and innervation of each specific muscle, as highlighted in our vintage anatomical study guide.
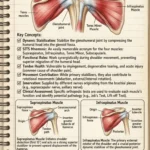
1. Supraspinatus Muscle The Supraspinatus sits right at the top of the shoulder and is the most commonly injured muscle of the rotator cuff.
- Origin: Supraspinous fossa of the scapula.
- Insertion: Superior facet of the greater tubercle of the humerus.
- Primary Action: It initiates shoulder abduction (lifting the arm away from the body) for the first 15 degrees. More importantly, it acts as a strong superior stabilizer, preventing the deltoid muscle from simply pulling the humerus straight up into the acromion during arm elevation.
- Innervation: Suprascapular nerve.
2. Infraspinatus Muscle Located on the back of the shoulder blade, this thick, triangular muscle is a powerhouse for outward rotation.
- Origin: Infraspinous fossa of the scapula.
- Insertion: Middle facet of the greater tubercle of the humerus.
- Primary Action: It is the primary external (lateral) rotator of the shoulder. It also provides crucial posterior dynamic stability to the glenohumeral joint.
- Innervation: Suprascapular nerve.
3. Teres Minor Muscle This narrow, elongated muscle sits just below the Infraspinatus and works very closely with it.
- Origin: Lateral border of the scapula (posterior surface).
- Insertion: Inferior facet of the greater tubercle of the humerus.
- Primary Action: It acts as a synergist to the Infraspinatus, assisting in external rotation and providing additional posterior stability to hold the humeral head in place.
- Innervation: Axillary nerve.
4. Subscapularis Muscle The Subscapularis is the outlier of the group. While the other three muscles sit on the back (posterior) or top (superior) of the shoulder blade, the Subscapularis is hidden on the front.
- Origin: Subscapular fossa (the anterior surface of the scapula that rests against the ribcage).
- Insertion: Lesser tubercle of the humerus.
- Primary Action: It is the primary internal (medial) rotator of the shoulder and the only rotator cuff muscle to attach to the lesser tubercle. It prevents anterior subluxation (forward dislocation) of the humeral head.
- Innervation: Upper and lower subscapular nerves.
Clinical Correlates: Why Rotator Cuffs Fail
Understanding the textbook anatomy of the SITS muscles is only half the battle. You must also understand how they fail in a clinical setting.
Rotator Cuff Impingement Syndrome Notice the anatomical space above the Supraspinatus tendon, beneath the coracoacromial arch. This space is extremely tight. If the biomechanics of the shoulder are altered (due to poor posture, repetitive overhead motion, or bone spurs), the Supraspinatus tendon can get pinched or “impinged” between the humeral head and the acromion, causing severe pain and inflammation.
Rotator Cuff Tears Tendon health is highly vulnerable in this region. Tears can be acute (from a sudden trauma or heavy lifting) or degenerative (wearing down over time due to age or chronic impingement). Because the Supraspinatus tendon has a zone of poor blood supply near its insertion point, it is notoriously the most frequent site of tearing.
Clinical Assessments Orthopedic specialists and physical therapists use specific tests to isolate and evaluate each muscle:
- Jobe’s Test (Empty Can Test): Used to isolate and test for Supraspinatus pathology.
- External Rotation Resistance: Tests the Infraspinatus and Teres Minor.
- Lift-Off Test: Specifically isolates the Subscapularis.
Conclusion
The dynamic stabilization provided by the Rotator Cuff is nothing short of incredible. The SITS muscles work synergistically during every arm movement, constantly adjusting tension to keep the humeral head perfectly centered in the shallow glenoid fossa.
By utilizing visual study guides like our vintage color-coded anatomical chart, memorizing complex relationships like origins, insertions, and clinical testing becomes vastly easier.
Bookmark this guide for your next anatomy exam or clinical rotation, and explore BodyPartArchive for more high-yield visual cheat sheets designed to make mastering human anatomy effortless.