Mastering Female Reproductive Anatomy: The Ultimate Visual Guide
The internal female reproductive system is an incredible network of organs perfectly engineered for gamete production, hormonal regulation, and facilitating the miracle of gestation. However, for medical, nursing, and biology students, mastering this complex interplay of anatomical structures and hormonal feedback loops can be incredibly daunting.
From understanding exactly where fertilization takes place to tracking the 28-day uterine cycle, there is a massive amount of high-yield information to memorize. Today, we are breaking down the central components—the uterus, ovaries, and uterine tubes—using our beautifully detailed, vintage-style anatomical cheat sheet.
The Central Hub: Anatomy of the Uterus
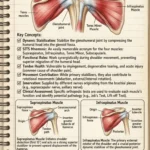
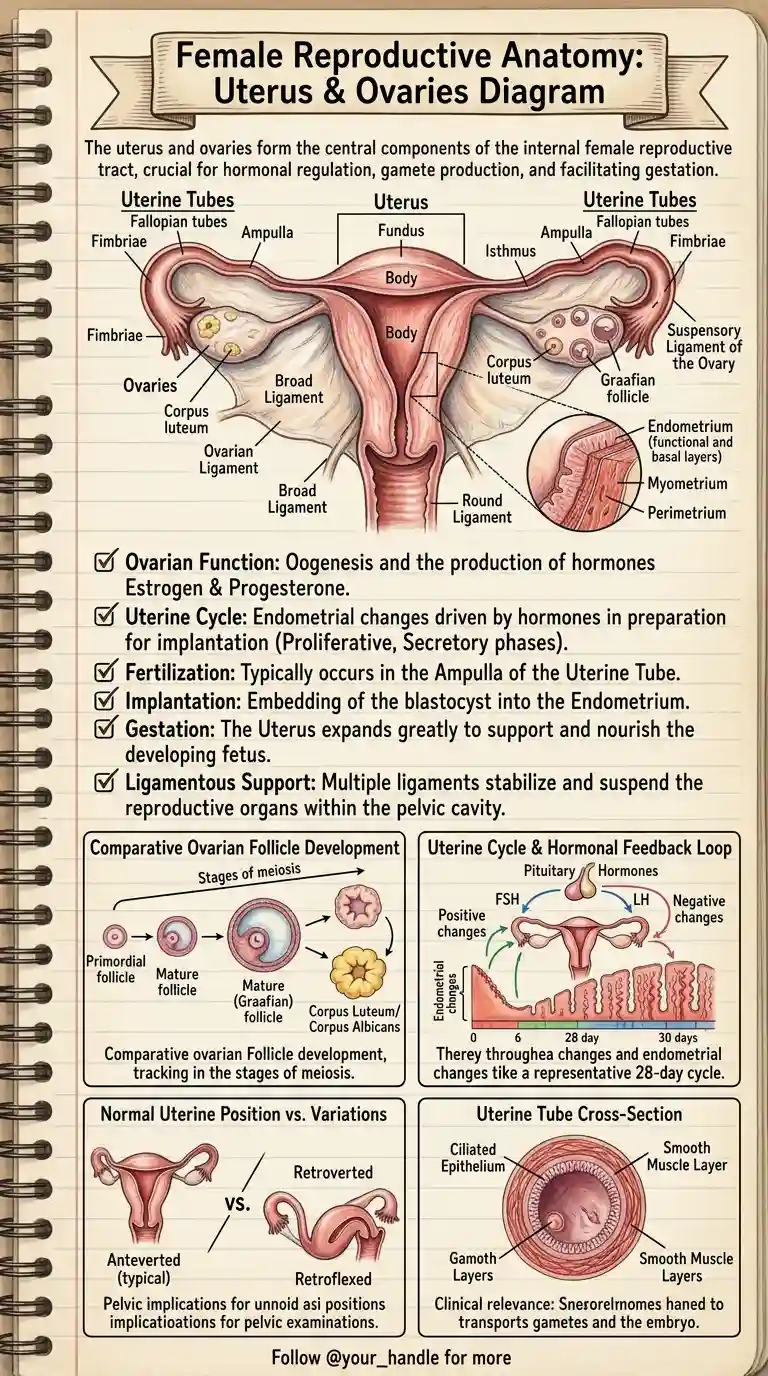
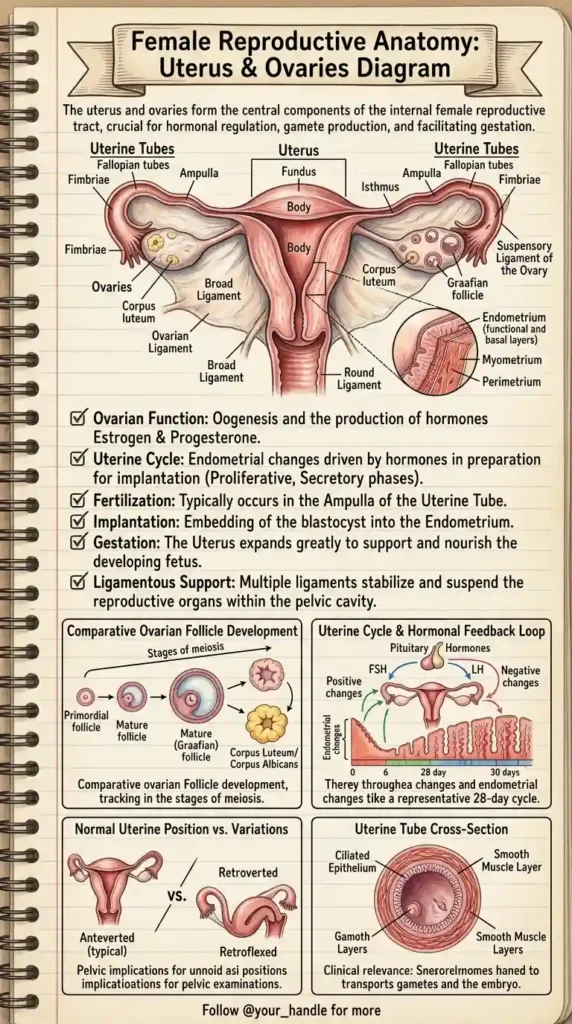
The uterus is a hollow, muscular, pear-shaped organ situated in the pelvic cavity. Its primary function is to accept a fertilized ovum, which implants into the inner wall, and to expand greatly to support and nourish a developing fetus during gestation.
Anatomically, the uterus is divided into distinct regions:
- The Fundus: The superior, dome-shaped portion located above the entry points of the uterine tubes.
- The Body (Corpus): The main, central portion of the uterus.
- The Isthmus: The narrow transition zone between the body and the cervix (the lower neck of the uterus that opens into the vagina).
The Three Layers of the Uterine Wall: To understand the uterine cycle, you must understand its microscopic layers:
- Perimetrium: The outermost protective serous layer.
- Myometrium: The thick middle layer consisting of interwoven smooth muscle fibers. This layer is responsible for the powerful contractions during labor.
- Endometrium: The highly vascular inner mucous membrane. This is the layer that thickens during the menstrual cycle in preparation for implantation. It consists of a functional layer (which sheds during menstruation) and a basal layer (which regenerates the functional layer).
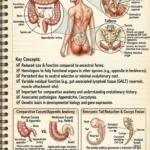
The Uterine Tubes (Fallopian Tubes)
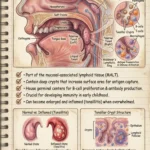
The uterine tubes extend laterally from the uterus and serve as the transport mechanism for the ovum (egg) and the site of fertilization.
- Fimbriae: These finger-like projections at the end of the tube sweep over the ovary to “catch” the released egg during ovulation.
- Ampulla: The widest and longest portion of the tube. High-Yield Fact: The ampulla is the most common site where fertilization of the egg by a sperm cell actually occurs.
- Cross-Sectional Anatomy: The inner lining of the tubes contains a ciliated epithelium. These microscopic hair-like structures, combined with the rhythmic contractions of the smooth muscle layers, gently transport the egg (or embryo) toward the uterus.
The Ovaries and Follicle Development
The ovaries are paired, almond-shaped glands responsible for oogenesis (the production of gametes/eggs) and the secretion of the primary female sex hormones: estrogen and progesterone.
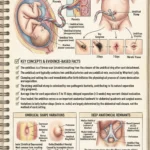
Comparative Ovarian Follicle Development: Within the ovaries, eggs develop inside protective fluid-filled sacs called follicles. The development tracks the stages of meiosis:
- Primordial Follicles: The resting stage of follicles present since birth.
- Mature (Graafian) Follicle: Driven by hormones, a follicle matures and bursts open during ovulation to release the egg.
- Corpus Luteum: After releasing the egg, the ruptured follicle transforms into the corpus luteum, a temporary endocrine structure that secretes progesterone to maintain the uterine lining for potential pregnancy. If no implantation occurs, it degenerates into the scar-like Corpus Albicans.
The Hormonal Feedback Loop and Uterine Cycle
The ovarian and uterine cycles are perfectly synchronized by a complex hormonal feedback loop between the brain (pituitary gland) and the reproductive organs.
- FSH (Follicle-Stimulating Hormone) & LH (Luteinizing Hormone): Secreted by the pituitary gland. FSH drives the maturation of the follicles in the ovary, while a sudden surge in LH triggers ovulation.
- The Uterine (Menstrual) Cycle: Representing a typical 28-day cycle, the endometrium undergoes distinct changes. Estrogen from the growing follicles drives the Proliferative Phase (thickening the lining). After ovulation, progesterone from the corpus luteum drives the Secretory Phase (making the lining nutrient-rich). If fertilization does not occur, hormone levels drop, leading to the shedding of the lining (Menstruation).
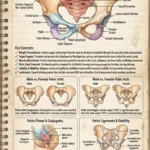
Ligamentous Support and Uterine Variations
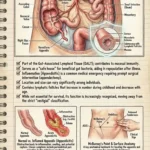
The reproductive organs do not just float freely; they are suspended and stabilized within the pelvic cavity by a complex system of ligaments:
- Broad Ligament: A wide fold of the peritoneum that drapes over the uterus and tubes like a sheet.
- Round Ligament: Binds the anterior of the uterus to the pelvic wall.
- Suspensory & Ovarian Ligaments: Anchor the ovaries in place.
Normal Uterine Position vs. Variations: Clinically, the position of the uterus is highly relevant during pelvic examinations. While the typical position is Anteverted (tilted forward over the bladder), many women have a Retroverted (tilted backward towards the rectum) or Retroflexed (bent backward) uterus. These are generally normal anatomical variations but are crucial to note for clinical charting.
Conclusion
Female reproductive anatomy is a symphony of dynamic structures and hormones. By using a visual study guide, the complex relationships between the pituitary hormones, ovarian follicles, and endometrial layers become significantly easier to comprehend and memorize.
Save this vintage anatomical guide to your study notes, and be sure to check back at BodyPartArchive for more high-yield visual cheat sheets designed to help you ace your medical exams!